Diabetic Eye Disease
If you have diabetes mellitus, your body does not use and store sugar properly. High blood sugar levels can damage blood vessels in the retina, the nerve layer at the back of the eye that senses light and helps to send images to the brain. The damage to retinal vessels is referred to as diabetic retinopathy.
Type of diabetic retinopathy
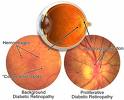
There are two types of diabetic retinopathy: nonproliferative diabetic retinopathy (NPDR) and proliferative diabetic retinopathy (PDR).
NPDR, commonly know as "background retinopathy," is an early stage of diabetic retinopathy. In this stage, tiny blood vessels with the retina leak blood or fluid. The leaking fluid causes the retina to swell or to form deposits called exudates. Many people with diabetes have mild NPDR, which usually does not affect their vision. When vision is affected it is the result of macular edema and / or macular ischemia.
Macular edema is swelling, or thickening, of the macula, a small area in the center of the retina that allows us to see fine details clearly. The swelling is caused by fluid leaking from retina blood vessels. It is the most common cause of visual loss in diabetes. Vision loss may by mild to severe, but even in the worst cases, peripheral vision continues to function.
Macular ischemia occurs when small blood vessels (capillaries) close. Vision blurs because the macula no longer receives sufficient blood supply to work properly.
PDR is present when abnormal new vessels (neovascularization) begin growing on the surface of the retina or optic nerve. The main cause of PDR is widespread closure of retinal blood vessels, preventing adequate blood flow. The retina responds by growing new blood vessels in an attempt to supply blood to the area where the original vessels closed.
Unfortunately, the new, abnormal blood vessels do not resupply the retina with normal blood flow. The new vessels are often accompanied by scar tissue that may cause wrinkling or detachment of the retina.
PDR may cause more severe vision loss than NPDR because it can affect both central and peripheral vision.
Proliferative diabetic retinopathy causes visual loss in the following ways:
Vitreous hemorrhage: The fragile new vessels may bleed into the vitreous, a clear jelly-like substance that fills the center of the eye. If the vitreous hemorrhage is small, a person might see only a few new dark floaters. A very large hemorrhage might block out all vision.
|